My appreciation is that the data taken as a whole constitutes proof. Absolute proof? Well, there's almost no such thing in Science. Definitely not. Proof beyond "reasonable doubt"? Taking all the evidence together, I think so, yes. Proof "on the balance of probability"? Certainly, that was found by the Full Bench of the Australian Family Court as far back as 2003, when there was far less evidence than today.
But what about taking each piece of evidence individually, on its own? Is there a single, reliable touchstone? Adequate for a diagnosis, as conjectured by a New Scientist article I blogged about a month ago?
Er.... I don't think so, no. Much as I'd like to believe otherwise.
To illustrate the limits of reliability of each individual piece of evidence taken on its own, there's a marvellous post that explains it far better than I could, on Sugar and Slugs: Why Sex Differences Don’t Always Measure Up.
Please read the whole thing. I'll just give some pictorial hints. First, some graphs showing the overlaps involved. To start with, nothing controversial: just height.

Then what I consider the single best piece of evidence, numbers and types of cells in one particular area of the brain.
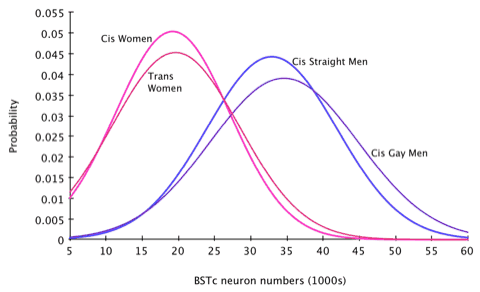
Well, so far, so good. There's overlap, but no worse than for height, and it's accepted without demur that "women are shorter than men" even though we all know many exceptions.
The one that illustrates graphically the problem we have regarding reliability is this:
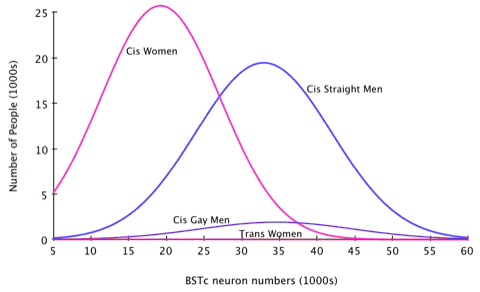
On the "number of cases examined" axis, we flatline. The difference from zero is too small to see at this resolution, we've lost all data.
We can be really certain about men and women in general, but for trans people, not so much.
Why?
First - there aren't that many Transsexuals. 1 in 3000 people or so.
Second - in medicine and psychology, many propositions have been accepted not so much as "True" as "True Enough". We routinely prescribe and conduct surgery on the basis of propositions only proven to the level of 0.05. Meaning there's a 1 in 20 chance we're wrong. This "medical standard of proof", once determined, is deemed enough - and getting funding just to remove a bit of doubt from something "everyone already knows" is problematic. Add in the fact that the test involves autopsying well-preserved brains of trans people, and repeated experiments here just aren't going to happen.
fMRI and PET scans don't have this disadvantage, so while the overlap there is greater, and the fuzziness more fuzzy, we can get better reliability by repeating things hundreds or thousands of times without requiring the subject to be dead.
Which is good for Science, but for diagnostic tests? When there's so much overlap in individuals and so much uncertainty on single measurements? No. Not enough. It might help, but a definitive test it's not, and on its own never will be.
A series of different, independant tests of the same kind might though. If each test has a 50% chance of being wrong, and we do 10 different tests, all saying the same thing... then the odds of being wrong are less than 1 in 1000.

18 comments:
'tis simple actually........before it was clear who was and wasn't born transsexed. Today you have a tonne of idiots claiming transsexuality who clearly do not fit the bill and researcher must separate them out to get decent data.
I submit your buddy Sandeen as representive of the problem.
Diagnosis might also be much easier if there was something with a known causal relation to transsexuality, not just correlation. Using any of these is a bit like trying to determine the sex of someone by measuring their height...
Cathryn - congrats once more on your win against one of the more egregiously obvious cases of religious bigotry I've ever seen. Your courage and fortitude is inspirational.
The Gloating Lamp is lit. Gloating is permitted, even to a completely unseemly extent, just this once. You deserve it and far more.
And you're right to a great degree: separating out people who are on the margins - Intersexed people like you or I - from non-IS TS to get a clean sample is difficult. Then there are those who are arguably not TS at all for other reasons.
I'd like to see data from non-ops as opposed to, um, ops. See if we can see which parts of the brain they differ in. Then those of the girlie girls vs the tomboys and geekettes like me.
I bet the difference there is larger, but involves the white matter and cortex rather than the lymbic system.
There is no such thing as a "male brain" or "female brain", only brains with different parts that are more or less feminised or masculinised to a greater or lesser degree.
Women have certain parts strongly feminised. They usually have most other parts feminised too. But all that's necessary for them to be called "women" is for one complex to be feminised. I don't think that complex necessarily includes the parts determining body map. Others differ there.
The calculation of the chance of a false result is correct if the results are uncorrelated. If they are correlated then the chance of an error is higher. If they are all perfectly correlated then the chance of an error is still 50%.
And of course, if it turns out it really is a physical brain factor, then TS could just be a kind of "invisible" IS condition...
I hate those pop science books that declare Women Are Like This, Men Are Like That. I'm not particularly femme, I'm not butch, I don't identify with most of the stereotypically male stuff in those books and often connect more with the stuff that's supposedly female, but I'm not trans. I'm okay with being seen as male, I'm okay with wearing a male body. If I'd been born into a female body I suspect that would have been okay with me, too. There were times as a child I was called a girl and my friendly phone voice can be mistaken for a woman's. This has only bothered me when it has bothered other people. When once in a customer service job the caller, hearing my name, said, "Like Glenn Close," I responded, "Among others Glenns."
Hi Glenn. You're not unique. You're not even unusual. Evidence from cases of Intersex suggest that perhaps one person in 3 feels as you do, to a greater or lesser extent.
See my post BiGender and the Brain
@Cathryn: On what grounds do you argue that (I presume) Autumn Sandeen is not transsexual?
I realize that she has done quite a number of things politically that have upset various factions among the trans community as a whole, but I must admit I'm a little puzzled by your assertion on this matter.
Given that activity strengthens brain connections, I would be very interested to know to what extent these differences exist at birth.
Does a typical cis woman have a female brain because she was born with one or because, having been born with female genitalia, she was encouraged to act female and by acting female developed a female brain?
(I am aware that neither "female brain" nor "act female" are technically/politically correct but it is a useful shorthand: with all the qualifications and weasel words the previous sentence would be 2000 words long and practically impossible to read)
Major - there's no solid evidence that post-natal environment has any influence.
We can definitely prove that it doesn't in CAH women, who show "masculine" play patterns even if strongly encouraged to be more feminine.
See this post and this one.
Mothers and fathers encouraged sex-typical toy play in children with and without CAH. However, girls with CAH received more positive feedback for play with girls' toys than did unaffected girls. Data show that increased male-typical toy play by girls with CAH cannot be explained by parental encouragement of male-typical toy play. Although parents encourage sex-appropriate behavior, their encouragement appears to be insufficient to override the interest of girls with CAH in cross-sexed toys.
(I am aware that neither "female brain" nor "act female" are technically/politically correct but it is a useful shorthand: with all the qualifications and weasel words the previous sentence would be 2000 words long and practically impossible to read)
3000+. But well said, we'll take them as read.
In Dr. Lawrence's CV there is a listing that she is preparing a manuscript
on the critique of the brain sex theory of transsexualism. This seems to be an update to the error filled one that she published online and the one where I followed it up with my own online article
about her straw man argument. I think that
in her new critique which she is going to try to submit to a peer review journal that she is going to try to state that NONE of the brains sex in transsexual papers have been replicated.
That no independent lab has replicated Swaab's results. That no independent lab has replicated the Savic PET scan studies. That no independent lab has replicated the fMRI work. That no independent lab has replicated the MRI work on the Putamen and that no independent lab has replicated the work
on DTI from Spain. I have been following the sexual orientation of the subjects (even to receiving personal communication from authors). It doesn't seem that sexual orientation of the subjects can be divided into a "homosexual" or "autogyenphilic" group.
The replication issue is the only one which she MAY be able to assert.
(I say may because I believe that replication studies are under way).
Any comments?
If her paper acts as a spur to get more data on the subject, that's all to the good.
Yes, it will be (mis)used for propaganda purposes, as her other papers were. She's great at data collection, terrible at analysis.
But the point is, we *do* need more independent confirmation. I think there's enough in aggregate now to be certain: but I'd like each individual data point to be shored up with more experiments.
Now if she only applied the same standards to AGP theory, which is the purest phlogiston. Then again, most psychology based on behavioural questioning is.
As someone who is 6'8", charts like these depress me sometimes :)
- Kath
Some girls would love to be 5'20".
Hugs, OK?
Keep in mind, a lot of non op people are none opp because of poverty, lack of insurance, concerns about the viability of the surgery, and some cases out of deep realistic concerns about safety and the price they will pay for the choice. And many who weren't impoverished before, become so after, having spent all they had and then losing everything else - transwomen in particular. Also, its a huge huge life decision and its pretty darned irreversible in many particulars. Some people struggle and waver for years, with enormous societal pressure and sheer horror of abuse and financial disaster staring them in the face...and its hell every second. Do not write off the non op corner of the world. Every individual has their own story. There are somethings that cannot be graphed no matter how hard we try, that remain reality.
Thanks for the linkage to my blog, I'm glad you liked the article.
You conclude saying:
A series of different, independent tests of the same kind might though. If each test has a 50% chance of being wrong, and we do 10 different tests, all saying the same thing... then the odds of being wrong are less than 1 in 1000.
It's true that if someone gets all ten right, the odds of it being a false positive are 1 in 1024. But if we were to only have ten tests, the odds of a true positive are also only 1 in 1024 because the test has to never screw up (see wolfram alpha for the distribution).
To actually recognize almost 90% of the target group, you need to say that they must pass ten tests out of twenty-five.
And this supposes that we can come up with sixteen statistically independent tests. In reality, many of the tests we might come up with are likely to depend on the same hidden variables.
(On the same day as your post, I added a comment to my own article talking about this issue, but it may not have been there when you read it. My numbers there are't quite as bad because I used the BSTc test as my example.)
> The replication issue is the only one which she MAY be able to assert.
Its a non issue. I said it in a lot of discussions. Each fMRT studies findings are confirmations of the earlier done research without actually doing the same.
Post a Comment